Please see letter for appointment details
Please telephone the Endoscopy department on 01234 792269 if this is not convenient for you.
Please contact 07392 126603 If you would like to discuss any aspects of the procedure before your appointment.
If you have not attended a Pre Assessment appointment you will receive a phone call for you to be pre assessed over the phone. This may come through as an unknown number.
Introduction
You have been advised by your GP or hospital doctor to have an investigation known as a ERCP. We will need to have your informed and signed consent before we can carry out this examination. This leaflet explains how the examinations are carried out and what the risks are. This will help you to make an informed decision when agreeing to the examinations.
What is an ERCP?
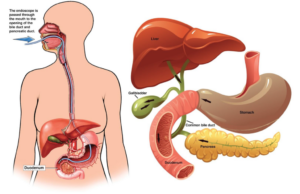
The examination you will be having is called an ERCP which stands for Endoscopic Retrograde Cholangio- Pancreatography. This procedure enables the doctor to examine the common bile duct and the pancreatic duct. The instrument used is a long, flexible tube about the same thickness as your finger with a light on the end called a duodenoscope. It also has a very small camera which sends a live image to a screen, where it is viewed by the doctor. The examination is carried out by a specially trained doctor called an endoscopist. During the ERCP, the endoscopist will also use X-rays and a special dye to show up your bile ducts on the screen.
In order to carry out this procedure the duodenoscope will be passed through your mouth down into the stomach and the first part of your small bowel (the duodenum) at the point where the bile duct and pancreatic duct drain into the small bowel.
ERCP is used mostly to diagnose and treat conditions of the bile ducts and pancreas.
Why do I need an ERCP? What are the benefits?
Your doctor is concerned that you may have problem or a blockage in your bile duct or pancreatic duct. Gallstones or narrowing in your bile duct are common problems, both which can cause jaundice (your eyes and skin turning yellow).
An ERCP may be recommended for a number of reasons, including to:
- Help your doctors to make a diagnosis.
- Treat jaundice caused by gallstones or narrowing of bile ducts
- Remove stones from the bile ducts or pancreatic ducts
- Insert a plastic or metal tube to drain the bile (or the pancreatic juices)
- Clear blockage of the bile flow
What are the risks and complications?
- Acute Pancreatitis: Injection of dye into the pancreatic duct can occasionally cause inflammation of the pancreas known as pancreatitis. The risk of this occurring is approximately 5%
- Bleeding: This can occur in 1 in 500 patients but is 10 times more likely (10 in 500) if a cut has been made (sphincterotomy) to remove stones or to insert a stent.If the x-rays show a gallstone the doctor will enlarge the opening of the bile duct (Sphincterotomy). This is done with an electrically heated wire (diathermy) which you will not feel. This procedure carries a 1% risk of significant bleeding but this risk is minimised by checking your blood clotting results before the procedure. If bleeding occurs, you may need a blood transfusion and very occasionally an operation to stop the bleeding.If a sphincterotomy is performed, pancreatitis may also occur, again with a risk of approximately 5%. If a narrowing is found, bile can be drained by leaving a short plastic tube (stent) in the bile duct. Occasionally it may be necessary to replace or remove the tube some months later if it becomes blocked.
- Perforation: A tear in the gastrointestinal wall or bile system occurs very rarely (1 in 1000 patients), which might require surgery to be repaired.
- Small abnormalities may be missed, although this is unlikely.
- Adverse reaction to the sedation medication or the X-ray dye.
- Short term problems with breathing, heart rate and blood pressure (related to sedation). You will be monitored closely so that if any problems do occur, they can be treated quickly.
- Heart attack or stroke (related to sedation)- though this is very unlikely
- Damage caused by the duodenoscope to teeth or bridgework– this is very rare
Please remember that these procedures and the risks are much safer than the only other option which is to have a full operation.
Are there any alternatives to an ERCP?
There are other ways of looking at your bile duct such as a Computed tomography (CT) and magnetic resonance imaging (MRI), or a technique called endoscopic ultrasound. These investigations can also provide pictures of internal organs and have a fewer complications but cannot be used to treat a problem, which an ERCP is often able to do. If you have a problem in your bile duct, an operation may be an alternative to an ERCP.
What will happen if I decide not to have an ERCP?
Your doctor may not be able to confirm or treat your problem. If you are concerned about having this procedure, you should discuss this with your doctor.
The Preparation
To allow a clear view into your stomach and small intestine (Duodenum) they must be empty, so it is important not to eat for 6 hours before your appointment. You can continue with sips of water up to 2 hours before your appointment time.
On the day of the procedure
When you arrive at Reception you will be asked to take a seat and wait to be called by the nurse who will explain the procedure and go through a series of questions about your general health. You will then be asked to get changed. The Endoscopist will go through a consent form with you and ask you to sign it. This is to ensure you understand the procedure and its implications and risks. If you have any worries or questions do not be afraid to ask. The staff want you to be relaxed as possible for the procedure and will not mind answering your queries. Please tell the nurse or doctor if you have had any reactions to drugs and any allergies you may have. You will need to remove any false teeth or contact lenses. Jewellery or metal objects must also be removed as they interfere with x-rays.
A small cannula will be inserted into a vein in your arm which allows access for the consultant to give you the sedative and any other medications that may be required.
During the Procedure
In the examination room you will be asked to lie on your stomach with your left arm down your side and your right arm up by your head, you will need to turn your head to face the right side. A small clip will be placed on your finger to monitor your pulse rate and oxygen levels during the procedure.
A small sponge will be placed just inside your nose to give you oxygen throughout the procedure and a mouth guard will be placed in your mouth to protect your teeth.
To ensure that you are relaxed and pain free you will receive a sedative and pain relieving injection which will make you sleepy.
The endoscope will be passed through your mouth down into the stomach and the first part of your small bowel (the duodenum) at the point where the bile duct and pancreatic duct drain into the small bowel. A dye which will show up on the x-rays, is injected via a small tube which will be passed through the endoscope, into the bile duct. Pictures can then be taken.
There are then a range of therapies that can be undertaken such as removal of Gall Stones and Stenting. The dye passes from your body harmlessly.
At the end of the procedure, you will be given a Diclofenac Suppository (anti-inflammatory) per rectum to reduce the risk of Pancreatitis. Please discuss this with your Endoscopist if you have any concerns.
Results
Before you leave the department, a nurse or doctor will explain the outcome of your procedure and discuss any changes of medication and further investigations or appointments you may require. Due to the effects of the sedation, many people find they forget everything that has been said to them. Your report will also be given to you in written form.
Going home
Once the examination has finished, you will go into our recovery area feeling sleepy. The nurses will advise you when you can eat and drink. You normally stay with us for approximately 4 hours post procedure depending on treatment during procedure. Once you have recovered from the procedure and sedation, the cannula will be removed and you will be able to get dressed. The nurse will also go through your report and the results of your procedure.
A nurse will take you to the Endoscopy discharge lounge and you will be given refreshments while you wait for your transport home. Once your escort has arrived to collect you from discharge lounge, your escort will need to sign the discharge form, being the responsible adult who will look after you in the next 12-24 hours.
Overall this is a safe procedure and most patients go home the same day.
Once home, it is important to rest quietly for the remainder of the day. The effects of the procedure and the sedation should have worn off by the next day, however the effects of the sedation can last for 24 hours, so for this time you must not:
- Drive a car;
- Operate machinery;
- Drink alcohol;
- Sign any legally binding documents;
- Be in charge of any young children.
You are advised against foreign/remote travel in the 2 week period after this procedure. Please discuss any concerns with the nursing team.
If there are any concerns at all about your condition after the procedure we will then keep you in hospital overnight to monitor your condition closely.
Points to Remember:
- If you are unable to keep your appointment please notify the Endoscopy unit as soon as possible
- It is our aim for you to be seen and investigated as soon as possible after your arrival. However the department is busy and your investigation may be delayed. If emergencies occur, these patients will obviously be given priority over less urgent cases.
- The hospital cannot accept any responsibility for the loss or damage of personal property during your time on these premises.
Concerns
If you have any queries regarding the procedure please contact the endoscopy unit between 8am and 6pm Monday to Sunday and the nursing staff will be happy to give you information or advice.
FOLLOWING THIS PROCEDURE YOU MUST NOT DONATE BLOOD FOR 4-6 MONTHS
The reason for this is that your ability to donate blood in the future is dependent upon your diagnosis and the possibility that you might need to undergo further investigations or complete treatments. (British Society of Gastroenterology, 2019)
Lifestyle changes
If you smoke, stopping smoking will improve your long-term health. Try to maintain a healthy weight. You have a higher risk of developing complications if you are overweight. Regular exercise should improve your long-term health. Before you start exercising, ask the healthcare team or your GP for advice.
Summary
An ERCP is usually a safe and effective way of treating a problem within your bile and pancreatic duct. However, complications can happen. You need to know about them to help you make an informed decision about the procedure. Knowing about them will also help to detect and treat any problems early.
Some information, such as risk and complication statistics, is taken from global studies and/or databases. Please ask your doctor for more information about the risks that are specific to you. This document is intended for information purposes only and should not replace advice that your relevant healthcare team would give you.
Additional Information
Having a procedure with a training endoscopist
Endoscopy Training at Bedford Hospital
Bedford Hospital contributes to the training of endoscopists and as a result has several trainees working in Endoscopy; this leaflet is provided to inform you about how this may affect your Endoscopy procedure, and support your decision as to whether you are happy to have a trainee perform the procedure.
Although the idea of a trainee may be unnerving it is often a very positive experience. All our Endoscopy trainees are in a structured training programme within the national guidelines.
Around a quarter of Endoscopy lists at Bedford Hospital involve training of endoscopists.
Will they be supervised?
Under no circumstances are trainee Endoscopists unsupervised. Depending on the experience of the trainee, the experienced Consultant or Senior Nurse Endoscopist will be present, and supervising your Endoscopy procedure throughout or will be immediately available in the endoscopy department. If at any time you or the trainee has any difficulties the trainer can intervene.
All the Endoscopy trainers at Bedford Hospital are accredited Endoscopy trainers and we regularly monitor their training skills.
Is it safe?
We carefully monitor our complication rates for Endoscopy and there is no difference in safety with a trainee Endoscopist.
Will it be more uncomfortable?
We carefully monitor patient comfort and have not found any suggestion it will be more uncomfortable.
Will it take longer?
While learning a trainee may be slower than an independent Endoscopist, however, our trainers are experienced in monitoring the length of a procedure and will take over if procedure seems prolonged. On a training list we allow a longer time for the whole Endoscopy experience, and patients often find this makes for a more relaxed atmosphere.
What should I do if I don’t want a trainee?
If you wish to let us know you are not happy to have a supervised trainee perform your procedure please inform us at least one week in advance of the procedure, so we can ensure you are not booked on a training list. The Endoscopy administrative team are on 01234 792269 or 01234 730567.